Patients with advanced arthritis of the hip may be candidates for either traditional total hip replacement or hip resurfacing. Each of these procedures is a type of hip replacement, but there are important differences. Your orthopedic surgeon will talk with you about the different procedures and which operation would be best for you.
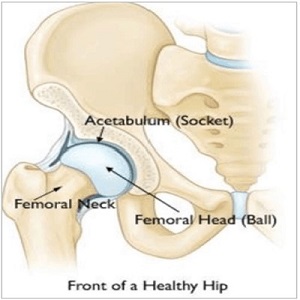 Front of healthy hip
Front of healthy hip
The hip is a ball-and-socket joint. In a healthy hip, the bones are covered with smooth cartilage that enables the femoral head and acetabulum to glide painlessly against each other.
Description
In a traditional total hip replacement, the head of the thighbone (femoral head) and the damaged socket (acetabulum) are both removed and replaced with metal, plastic, or ceramic components. In hip resurfacing, the femoral head is trimmed and capped with a smooth metal covering. The damaged bone and cartilage within the socket are removed and replaced with a metal shell, just as in a traditional total hip replacement.

(Left) In the x-ray of a hip resurfacing taken from the front, a metal cap now covers the femoral head, and a small stem is seen in the femoral neck. A metal socket is also in place. Unlike the traditional total hip replacement shown on the right, the femoral head and neck are not removed.
Advantages of Hip Resurfacing
The advantages of hip resurfacing over traditional total hip replacements are an area of controversy among orthopedic surgeons. A great deal of research is currently being done on this topic.
- Hip resurfacings may be easier to revise. Because the components (called implants) used in hip replacements and hip resurfacings are mechanical parts, they can — and do — wear out or loosen over time. This typically occurs between 10 and 20 years after the procedure, although implants may last longer or shorter periods of time.
- If an implant fails, an additional operation may be necessary. This second procedure is called a revision and it can be more complicated than the initial operation. Because hip resurfacing removes less bone from the femur (thighbone) than a traditional hip replacement, many surgeons believe it is easier to exchange implants that fail after hip resurfacing.
- Decreased risk of hip dislocation. In hip resurfacing, the size of the ball is larger than in a traditional hip replacement. Because of this, it may be harder to dislocate. This stance is controversial because several factors can affect the risk of dislocation, such as surgical approach, and the type and size of the implants used.
- More normal walking pattern. Some studies have shown that walking patterns are more natural following hip resurfacing compared to traditional hip replacement. These differences in walking are quite subtle, however, and special instruments are needed to measure them.
Disadvantages of Hip Resurfacing
- Femoral neck fracture. A small percentage of hip resurfacing patients will eventually break (fracture) the thighbone at the femoral neck. If this occurs, it is usually necessary to convert the hip resurfacing into a traditional hip replacement.
- A femoral neck fracture is not possible with a traditional hip replacement because the femoral neck is removed during this procedure. However, fractures around the implants can still occur with a traditional hip replacement.
- Metal ion risk. In hip resurfacing, a metal ball moves within a metal socket. Over time, this leads to the production of tiny metal particles called ions. Some patients may develop sensitivity or allergy to the metal particles, which may cause pain and swelling. Also, there are concerns that the metal particles may increase the risk of cancer, although this has never been proven. Some types of traditional hip replacements also consist of a metal ball and a metal socket and these replacements run the same potential risks. Ask your doctor for more information about metal-on-metal implants.
- Hip resurfacing is a more difficult operation. Hip resurfacings are more difficult than total hip replacements for surgeons to perform. As such, a larger incision is usually required for a hip resurfacing compared to a total hip replacement.
Candidates for Surgery
Your doctor may recommend surgery if you have more advanced osteoarthritis and have exhausted the nonsurgical treatment options. Surgery should only be considered if your hip is significantly affecting the quality of your life and interfering with your normal activities.
Unlike hip replacement, hip resurfacing is not suitable for all patients. Generally speaking, the best candidates for hip resurfacing are younger (less than 50), larger-framed patients (often, but not always male) with strong, healthy bone. Patients that are older, female, smaller-framed, with weaker or damaged bone are at higher risk of complications, such as femoral neck fracture and should be treated with total hip replacement.
Your Surgery
Before Surgery
Before your procedure, a doctor from the anesthesia department will evaluate you. He or she will review your medical history and discuss anesthesia choices with you. You should also have discussed anesthesia choices with your surgeon during your preoperative clinic visits. Anesthesia can be either general (you are put to sleep) or spinal (you are awake but your body is numb from the waist down).
Your surgeon will also see you before surgery and sign your hip to verify the surgical site.
Surgical Procedure
A hip resurfacing operation typically lasts between 1-2 hours.
Your surgeon will make an incision in your thigh in order to reach the hip joint. The femoral head is then dislocated out of the socket. Next, the head is trimmed with specially designed power instruments. A metal cap is cemented over the prepared femoral head. The cartilage that lines the socket is removed with a power tool called a reamer. A metal cup is then pushed into the socket and held in place by friction between the bone and the metal. Once the cup is in place, the femoral head is relocated back into the socket and the incision is closed. After the surgery you will be taken to the recovery room, where you will be closely monitored by nurses as you recover from the anesthesia. You will then either be discharged home or admitted to the hospital. Patients admitted to the hospital are usually discharged after a one-night stay.
Complications
As with any surgical procedure, there are risks involved with hip resurfacing. Your surgeon will discuss each of the risks with you and will take specific measures to help avoid potential complications.
Although rare, the most common complications of hip resurfacing are:
- Blood clots. Blood clots in the leg veins are the most common complication of hip resurfacing surgery. Blood clots can form in the deep veins of the legs or pelvis after surgery. Blood thinners such as warfarin (Coumadin), low-molecular-weight heparin, aspirin, or other drugs can help prevent this problem.
- Infection. You will be given antibiotics before and after your surgery to prevent infection.
- vessels may be injured or stretched during the procedure. Injury to nerves or vessels. Although it rarely happens, nerves or blood.
- Femoral neck fracture
- Dislocation
- Risks of anesthesia
Recovery
You may begin putting weight on your leg immediately after surgery, depending on your doctor’s preferences and the strength of your bone. You may need a walker, cane, or crutches for the first few weeks until you become comfortable enough to walk without assistance.
You can expect some pain and discomfort during the recovery period. Many types of pain medication are available to help control pain, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs) and local anesthetics. Treating pain with medications can help you feel more comfortable, which will help your body heal faster and recover from surgery faster.
Opioids can provide excellent pain relief; however, they are a narcotic and can be addictive. It is important to use opioids only as directed by your doctor. You should stop taking these medications as soon as your pain starts to improve. You will be given exercises to help maintain your range of motion and restore your strength.
